Do I Have Fallen Arches??
Overview

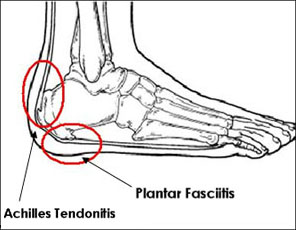
Fallen arches is a common term used to describe a flatfoot condition that develops during adulthood. This should not be confused with other causes of flatfoot that may develop during childhood or adolescence. Most cases of ?fallen arches? develop when the main arch-supporting tendon (the posterior tibial tendon) becomes weakened or injured, causing the arch to gradually become lower. With time, the shape of the foot changes and secondary symptoms start to appear. Common problems associated with fallen arches include plantar fasciitis, tendonitis, increased fatigue, and arthritis of the foot and ankle.
Causes
Turning 40 doesn?t necessarily have anything to do with it, but over time you?ve likely engaged in certain activities or developed some unhealthy habits that led to this condition. If you are overweight, you are placing excess burdens on your feet, causing the tendons to strain. Some women experience fallen arches because of weight gain during pregnancy. You also may have damaged these tendons while exercising. If you suffered a serious injury to the foot, you may have weakened the tendons, which can also lead to this development.
Symptoms
A symptom is something the patient feels and reports, while a sign is something other people, including the doctor may detect. An example of a symptom may be pain in the ankle, while a sign may be a swelling. Symptoms may vary and generally depend on the severity of the condition. Some have an uneven distribution of bodyweight and find that the heel of their shoes wears out more rapidly and more on one side than the other. The most common signs or symptoms of flat feet are pain in the ankle (inner side), there may also be swelling of the foot in general, swelling in the arch of the foot, the calf, knee, the hip, the back, the general lower leg area. People with flat feet may also experience stiffness in one or both feet. One or both feet may be flat on the ground (either no arch, or very slight arch). Shoes may wear unevenly.
Diagnosis
An examination of the foot is enough for the health care provider to diagnose flat foot. However, the cause must be determined. If an arch develops when the patient stands on his or her toes, the flat foot is called flexible and no treatment or further work-up is necessary. If there is pain associated with the foot or if the arch does not develop with toe-standing, x-rays are necessary. If a tarsal coalition is suspected, a CT scan is often ordered. If a posterior tibial tendon injury is suspected, your health care provider may recommend an MRI.
pes planus radiology
Non Surgical Treatment
Physiotherapists will carry out a detailed biomechanical assessment of your feet and lower limb. Once the causes have been identified a number of treatment methods may be used to help relieve pain and restore function in the feet including the use of custom made orthotics to support the foot and offload the areas which are painful, strengthening exercises for weakened muscles and tendons in the arch, and massage and mobilisation techniques to help mobilise stiff tissue and joints in the foot.
Surgical Treatment

Fallen arches may occur with deformities of the foot bones. Tarsal coalition is a congenital condition in which the bones of the foot do not separate from one another during development in the womb. A child with tarsal coalition exhibits a rigid flat foot, which can be painful, notes the patient information website eOrthopod. Surgery may prove necessary to separate the bones. Other foot and ankle conditions that cause fallen arches may also require surgery if noninvasive treatments fail to alleviate pain and restore normal function.
Fallen arches is a common term used to describe a flatfoot condition that develops during adulthood. This should not be confused with other causes of flatfoot that may develop during childhood or adolescence. Most cases of ?fallen arches? develop when the main arch-supporting tendon (the posterior tibial tendon) becomes weakened or injured, causing the arch to gradually become lower. With time, the shape of the foot changes and secondary symptoms start to appear. Common problems associated with fallen arches include plantar fasciitis, tendonitis, increased fatigue, and arthritis of the foot and ankle.
Causes
Turning 40 doesn?t necessarily have anything to do with it, but over time you?ve likely engaged in certain activities or developed some unhealthy habits that led to this condition. If you are overweight, you are placing excess burdens on your feet, causing the tendons to strain. Some women experience fallen arches because of weight gain during pregnancy. You also may have damaged these tendons while exercising. If you suffered a serious injury to the foot, you may have weakened the tendons, which can also lead to this development.
Symptoms
A symptom is something the patient feels and reports, while a sign is something other people, including the doctor may detect. An example of a symptom may be pain in the ankle, while a sign may be a swelling. Symptoms may vary and generally depend on the severity of the condition. Some have an uneven distribution of bodyweight and find that the heel of their shoes wears out more rapidly and more on one side than the other. The most common signs or symptoms of flat feet are pain in the ankle (inner side), there may also be swelling of the foot in general, swelling in the arch of the foot, the calf, knee, the hip, the back, the general lower leg area. People with flat feet may also experience stiffness in one or both feet. One or both feet may be flat on the ground (either no arch, or very slight arch). Shoes may wear unevenly.
Diagnosis
An examination of the foot is enough for the health care provider to diagnose flat foot. However, the cause must be determined. If an arch develops when the patient stands on his or her toes, the flat foot is called flexible and no treatment or further work-up is necessary. If there is pain associated with the foot or if the arch does not develop with toe-standing, x-rays are necessary. If a tarsal coalition is suspected, a CT scan is often ordered. If a posterior tibial tendon injury is suspected, your health care provider may recommend an MRI.
pes planus radiology
Non Surgical Treatment
Physiotherapists will carry out a detailed biomechanical assessment of your feet and lower limb. Once the causes have been identified a number of treatment methods may be used to help relieve pain and restore function in the feet including the use of custom made orthotics to support the foot and offload the areas which are painful, strengthening exercises for weakened muscles and tendons in the arch, and massage and mobilisation techniques to help mobilise stiff tissue and joints in the foot.
Surgical Treatment
Fallen arches may occur with deformities of the foot bones. Tarsal coalition is a congenital condition in which the bones of the foot do not separate from one another during development in the womb. A child with tarsal coalition exhibits a rigid flat foot, which can be painful, notes the patient information website eOrthopod. Surgery may prove necessary to separate the bones. Other foot and ankle conditions that cause fallen arches may also require surgery if noninvasive treatments fail to alleviate pain and restore normal function.
Do You Understand Heel Discomfort?
Overview
Heel pain is pain in the heel area that can vary in severity and location. It is most common in adults. The heel is the first bone to contact the ground when walking and takes the full force of impact and the resulting shock of bearing weight during motion.
Causes
There are several causes of heel pain. By far the most common cause in adults is a condition commonly known as plantar fasciitis. Other names occasionally used for the same condition are heel spurs, and policeman?s heel. Plantar means bottom of the foot, and fascia is the fibrous tissues that helps tether the heel bone (calcaneus) to the heads of the metatarsal bones found at the base of your toes The meaning of ?itis? is inflammation. However, inflammation does not have a large part to play in the pathology, it is more degenerative (wear & tear) so the preferred title is plantar fasciosis or plantar aponeurotic fasciosis. For simplicity sake, we will refer to this common cause of heel pain as plantar fasciitis in this manual.
Symptoms
Both heel pain and heel spurs are frequently associated with an inflammation of the long band of tissue that connects the heel and the ball of the foot. The inflammation of this arch area is called plantar fasciitis. The inflammation maybe aggravated by shoes that lack appropriate support and by the chronic irritation that sometimes accompanies an athletic lifestyle. Achilles Tendinopathy, Pain and inflammation of the tendon at the back of the heel that connects the calf muscle to the foot. Sever?s, Often found in children between the ages of 8 - 13 years and is an inflammation of the calcaneal epiphyseal plate (growth plate) in the back of the heel. Bursitis, An inflamed bursa is a small irritated sack of fluid at the back of the heel. Other types of heel pain include soft tissue growths, Haglunds deformity (bone enlargement at the back of the heel), bruises or stress fractures and possible nerve entrapment.
Diagnosis
Your doctor will listen to your complaints about your heel and examine you to see what is causing the pain, and whether anything else has started it off. If the cause of your pain seems obvious, your doctor may be happy to start treatment straight away. However, some tests may be helpful in ruling out other problems. Blood tests may be done for arthritis. An Xray will show any arthritis in the ankle or subtalar joint, as well as any fracture or cyst in the calcaneum. (It will also show a spur if you have one, but as we know this is not the cause of the pain.) Occasionally a scan may be used to help spot arthritis or a stress fracture.
Non Surgical Treatment
Orthotics, by treating the cause of the problem, lead to the cure bette than 90% of the time. A small number of patients have waited so long that the plantar fascia has become thickened and filled with scar tissue and are not helped by ?conventional? means. Those are the patients that have, traditionally, required surgical treatment in which the plantar fascia is cut off the heel bone. Luckily, most surgery has been replaced by a relatively new mode of treatment, ESWT or Extracorporeal Shockwave Therapy. ESWT involves the application of multiple shockwaves to the diseased tendon or ligament and has an approximately 85 to 90% success rate. Keep in mind we are talking about this success rate in patients who are ?tough cases,? that is, already had the conventional treatment. The ESWT machines look like miniature renal lithtripsors (kidney stone crushers). There are virtually no side effects to ESWT other than the price as only about 30% of insurance companies are paying for it. They realize that it is less costly and safer than surgery but also know that many more people who would avoid surgery would have no problem getting ESWT so the volume of services would go up. You don?t have to live with painful heels.
Surgical Treatment
If treatment hasn't worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints or a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as open surgery, where the section of the plantar fascia is released by making a cut into your heel or endoscopic or minimal incision surgery - where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team.
pain in back of heel
Prevention

Maintaining flexible and strong muscles in your calves, ankles, and feet can help prevent some types of heel pain. Always stretch and warm-up before exercising. Wear comfortable, properly fitting shoes with good arch support and cushioning. Make sure there is enough room for your toes.
Heel pain is pain in the heel area that can vary in severity and location. It is most common in adults. The heel is the first bone to contact the ground when walking and takes the full force of impact and the resulting shock of bearing weight during motion.
Causes
There are several causes of heel pain. By far the most common cause in adults is a condition commonly known as plantar fasciitis. Other names occasionally used for the same condition are heel spurs, and policeman?s heel. Plantar means bottom of the foot, and fascia is the fibrous tissues that helps tether the heel bone (calcaneus) to the heads of the metatarsal bones found at the base of your toes The meaning of ?itis? is inflammation. However, inflammation does not have a large part to play in the pathology, it is more degenerative (wear & tear) so the preferred title is plantar fasciosis or plantar aponeurotic fasciosis. For simplicity sake, we will refer to this common cause of heel pain as plantar fasciitis in this manual.
Symptoms
Both heel pain and heel spurs are frequently associated with an inflammation of the long band of tissue that connects the heel and the ball of the foot. The inflammation of this arch area is called plantar fasciitis. The inflammation maybe aggravated by shoes that lack appropriate support and by the chronic irritation that sometimes accompanies an athletic lifestyle. Achilles Tendinopathy, Pain and inflammation of the tendon at the back of the heel that connects the calf muscle to the foot. Sever?s, Often found in children between the ages of 8 - 13 years and is an inflammation of the calcaneal epiphyseal plate (growth plate) in the back of the heel. Bursitis, An inflamed bursa is a small irritated sack of fluid at the back of the heel. Other types of heel pain include soft tissue growths, Haglunds deformity (bone enlargement at the back of the heel), bruises or stress fractures and possible nerve entrapment.
Diagnosis
Your doctor will listen to your complaints about your heel and examine you to see what is causing the pain, and whether anything else has started it off. If the cause of your pain seems obvious, your doctor may be happy to start treatment straight away. However, some tests may be helpful in ruling out other problems. Blood tests may be done for arthritis. An Xray will show any arthritis in the ankle or subtalar joint, as well as any fracture or cyst in the calcaneum. (It will also show a spur if you have one, but as we know this is not the cause of the pain.) Occasionally a scan may be used to help spot arthritis or a stress fracture.
Non Surgical Treatment
Orthotics, by treating the cause of the problem, lead to the cure bette than 90% of the time. A small number of patients have waited so long that the plantar fascia has become thickened and filled with scar tissue and are not helped by ?conventional? means. Those are the patients that have, traditionally, required surgical treatment in which the plantar fascia is cut off the heel bone. Luckily, most surgery has been replaced by a relatively new mode of treatment, ESWT or Extracorporeal Shockwave Therapy. ESWT involves the application of multiple shockwaves to the diseased tendon or ligament and has an approximately 85 to 90% success rate. Keep in mind we are talking about this success rate in patients who are ?tough cases,? that is, already had the conventional treatment. The ESWT machines look like miniature renal lithtripsors (kidney stone crushers). There are virtually no side effects to ESWT other than the price as only about 30% of insurance companies are paying for it. They realize that it is less costly and safer than surgery but also know that many more people who would avoid surgery would have no problem getting ESWT so the volume of services would go up. You don?t have to live with painful heels.
Surgical Treatment
If treatment hasn't worked and you still have painful symptoms after a year, your GP may refer you to either an orthopaedic surgeon, a surgeon who specialises in surgery that involves bones, muscles and joints or a podiatric surgeon, a podiatrist who specialises in foot surgery. Surgery is sometimes recommended for professional athletes and other sportspeople whose heel pain is adversely affecting their career. Plantar release surgery is the most widely used type of surgery for heel pain. The surgeon will cut the fascia to release it from your heel bone and reduce the tension in your plantar fascia. This should reduce any inflammation and relieve your painful symptoms. Surgery can be performed either as open surgery, where the section of the plantar fascia is released by making a cut into your heel or endoscopic or minimal incision surgery - where a smaller incision is made and special instruments are inserted through the incision to gain access to the plantar fascia. Endoscopic or minimal incision surgery has a quicker recovery time, so you will be able to walk normally much sooner (almost immediately), compared with two to three weeks for open surgery. A disadvantage of endoscopic surgery is that it requires both a specially trained surgical team and specialised equipment, so you may have to wait longer for treatment than if you were to choose open surgery. Endoscopic surgery also carries a higher risk of damaging nearby nerves, which could result in symptoms such as numbness, tingling or some loss of movement in your foot. As with all surgery, plantar release carries the risk of causing complications such as infection, nerve damage and a worsening of your symptoms after surgery (although this is rare). You should discuss the advantages and disadvantages of both techniques with your surgical team.
pain in back of heel
Prevention
Maintaining flexible and strong muscles in your calves, ankles, and feet can help prevent some types of heel pain. Always stretch and warm-up before exercising. Wear comfortable, properly fitting shoes with good arch support and cushioning. Make sure there is enough room for your toes.
Functional Leg Length Discrepancy Running
Overview
Neuromuscular. Muscle imbalance causing different pull on pelvis (anterior superior Ilium or posterior inferior ilium). Muscle tightness/shortness especially piriformis (which lead to an external rotation of the femur thus shortening of the leg) and QL (raising ipsilateral iliac crest). Genu recurvatum, valgus, varus. Asymmetrical fallen arches or over pronation. Polio, Cerebral palsy. Trauma. Fracture. Injury epiphyseal plate. Iatrogenic (such as hip or knee surgery). Idiopathic. Hip disorder (such Legg-Perthes-Calve? or Slipped capital femoral epiphysis). Advanced degenerative changes.
Causes
Common causes include bone infection, bone diseases, previous injuries, or broken bones. Other causes may include birth defects, arthritis where there is a loss of articular surface, or neurological conditions.
Symptoms
The effects of a short leg depend upon the individual and the extent of discrepancy. The most common manifestation if a lateral deviation of the lumbar spine toward the short side with compensatory curves up the spine that can extend into the neck and even impacts the TMJ. Studies have shown that anterior and posterior curve abnormalities also can result.
Diagnosis
Limb length discrepancy can be measured by a physician during a physical examination and through X-rays. Usually, the physician measures the level of the hips when the child is standing barefoot. A series of measured wooden blocks may be placed under the short leg until the hips are level. If the physician believes a more precise measurement is needed, he or she may use X-rays. In growing children, a physician may repeat the physical examination and X-rays every six months to a year to see if the limb length discrepancy has increased or remained unchanged. A limb length discrepancy may be detected on a screening examination for curvature of the spine (scoliosis). But limb length discrepancy does not cause scoliosis.
Non Surgical Treatment
In order to measure for correction, use a series of blocks or sheets of firm material (cork or neoprene) of varying thickness, e.g., 1/8", 1/4", and 1/2". Place them under the short limb, either under the heel or the entire foot, depending on the pathology, until the patient feels most balanced. Usually you will not be able to correct for the full amount of the imbalance at the outset. The longer a patient has had the LLD, the less likely he or she will be able to tolerate a full correction immediately. This is a process of incremental improvements. 2 inch External Platform Lift Bear in mind that the initial lift may need to be augmented as the patient's musculoskeletal system begins to adjust. It is often recommended that the initial buildup should be 50 percent of the total. After a suitable break-in period, one month say, another 25 percent can be added. If warranted, the final 25 percent can be added a month later. Once you determine how much lift the patient can handle, you then need to decide how to best apply it. There are certain advantages and disadvantages to using either internal or external heel lifts.

height increase medicine
Surgical Treatment
Surgical operations to equalize leg lengths include the following. Shortening the longer leg. This is usually done if growth is already complete, and the patient is tall enough that losing an inch is not a problem. Slowing or stopping the growth of the longer leg. Growth of the lower limbs take place mainly in the epiphyseal plates (growth plates) of the lower femur and upper tibia and fibula. Stapling the growth plates in a child for a few years theoretically will stop growth for the period, and when the staples were removed, growth was supposed to resume. This procedure was quite popular till it was found that the amount of growth retarded was not certain, and when the staples where removed, the bone failed to resume its growth. Hence epiphyseal stapling has now been abandoned for the more reliable Epiphyseodesis. By use of modern fluoroscopic equipment, the surgeon can visualize the growth plate, and by making small incisions and using multiple drillings, the growth plate of the lower femur and/or upper tibia and fibula can be ablated. Since growth is stopped permanently by this procedure, the timing of the operation is crucial. This is probably the most commonly done procedure for correcting leg length discrepancy. But there is one limitation. The maximum amount of discrepancy that can be corrected by Epiphyseodesis is 5 cm. Lengthening the short leg. Various procedures have been done over the years to effect this result. External fixation devices are usually needed to hold the bone that is being lengthened. In the past, the bone to be lengthened was cut, and using the external fixation device, the leg was stretched out gradually over weeks. A gap in the bone was thus created, and a second operation was needed to place a bone block in the gap for stability and induce healing as a graft. More recently, a new technique called callotasis is being use. The bone to be lengthened is not cut completely, only partially and called a corticotomy. The bone is then distracted over an external device (usually an Ilizarov or Orthofix apparatus) very slowly so that bone healing is proceeding as the lengthening is being done. This avoids the need for a second procedure to insert bone graft. The procedure involved in leg lengthening is complicated, and fraught with risks. Theoretically, there is no limit to how much lengthening one can obtain, although the more ambitious one is, the higher the complication rate.
Neuromuscular. Muscle imbalance causing different pull on pelvis (anterior superior Ilium or posterior inferior ilium). Muscle tightness/shortness especially piriformis (which lead to an external rotation of the femur thus shortening of the leg) and QL (raising ipsilateral iliac crest). Genu recurvatum, valgus, varus. Asymmetrical fallen arches or over pronation. Polio, Cerebral palsy. Trauma. Fracture. Injury epiphyseal plate. Iatrogenic (such as hip or knee surgery). Idiopathic. Hip disorder (such Legg-Perthes-Calve? or Slipped capital femoral epiphysis). Advanced degenerative changes.
Causes
Common causes include bone infection, bone diseases, previous injuries, or broken bones. Other causes may include birth defects, arthritis where there is a loss of articular surface, or neurological conditions.
Symptoms
The effects of a short leg depend upon the individual and the extent of discrepancy. The most common manifestation if a lateral deviation of the lumbar spine toward the short side with compensatory curves up the spine that can extend into the neck and even impacts the TMJ. Studies have shown that anterior and posterior curve abnormalities also can result.
Diagnosis
Limb length discrepancy can be measured by a physician during a physical examination and through X-rays. Usually, the physician measures the level of the hips when the child is standing barefoot. A series of measured wooden blocks may be placed under the short leg until the hips are level. If the physician believes a more precise measurement is needed, he or she may use X-rays. In growing children, a physician may repeat the physical examination and X-rays every six months to a year to see if the limb length discrepancy has increased or remained unchanged. A limb length discrepancy may be detected on a screening examination for curvature of the spine (scoliosis). But limb length discrepancy does not cause scoliosis.
Non Surgical Treatment
In order to measure for correction, use a series of blocks or sheets of firm material (cork or neoprene) of varying thickness, e.g., 1/8", 1/4", and 1/2". Place them under the short limb, either under the heel or the entire foot, depending on the pathology, until the patient feels most balanced. Usually you will not be able to correct for the full amount of the imbalance at the outset. The longer a patient has had the LLD, the less likely he or she will be able to tolerate a full correction immediately. This is a process of incremental improvements. 2 inch External Platform Lift Bear in mind that the initial lift may need to be augmented as the patient's musculoskeletal system begins to adjust. It is often recommended that the initial buildup should be 50 percent of the total. After a suitable break-in period, one month say, another 25 percent can be added. If warranted, the final 25 percent can be added a month later. Once you determine how much lift the patient can handle, you then need to decide how to best apply it. There are certain advantages and disadvantages to using either internal or external heel lifts.
height increase medicine
Surgical Treatment
Surgical operations to equalize leg lengths include the following. Shortening the longer leg. This is usually done if growth is already complete, and the patient is tall enough that losing an inch is not a problem. Slowing or stopping the growth of the longer leg. Growth of the lower limbs take place mainly in the epiphyseal plates (growth plates) of the lower femur and upper tibia and fibula. Stapling the growth plates in a child for a few years theoretically will stop growth for the period, and when the staples were removed, growth was supposed to resume. This procedure was quite popular till it was found that the amount of growth retarded was not certain, and when the staples where removed, the bone failed to resume its growth. Hence epiphyseal stapling has now been abandoned for the more reliable Epiphyseodesis. By use of modern fluoroscopic equipment, the surgeon can visualize the growth plate, and by making small incisions and using multiple drillings, the growth plate of the lower femur and/or upper tibia and fibula can be ablated. Since growth is stopped permanently by this procedure, the timing of the operation is crucial. This is probably the most commonly done procedure for correcting leg length discrepancy. But there is one limitation. The maximum amount of discrepancy that can be corrected by Epiphyseodesis is 5 cm. Lengthening the short leg. Various procedures have been done over the years to effect this result. External fixation devices are usually needed to hold the bone that is being lengthened. In the past, the bone to be lengthened was cut, and using the external fixation device, the leg was stretched out gradually over weeks. A gap in the bone was thus created, and a second operation was needed to place a bone block in the gap for stability and induce healing as a graft. More recently, a new technique called callotasis is being use. The bone to be lengthened is not cut completely, only partially and called a corticotomy. The bone is then distracted over an external device (usually an Ilizarov or Orthofix apparatus) very slowly so that bone healing is proceeding as the lengthening is being done. This avoids the need for a second procedure to insert bone graft. The procedure involved in leg lengthening is complicated, and fraught with risks. Theoretically, there is no limit to how much lengthening one can obtain, although the more ambitious one is, the higher the complication rate.
Mortons Neuroma Treatment
Overview
 Morton's neuroma, also called Morton's metatarsalgia, Morton's disease, Morton's neuralgia, Morton metatarsalgia, Morton nerve entrapment, plantar neuroma, or intermetatarsal neuroma is a benign (non-cancerous) growth of nerve tissue (neuroma) that develops in the foot, usually between the third and fourth toes (an intermetatarsal plantar nerve, most commonly of the third and fourth intermetatarsal spaces). It is a common, painful condition.
Morton's neuroma, also called Morton's metatarsalgia, Morton's disease, Morton's neuralgia, Morton metatarsalgia, Morton nerve entrapment, plantar neuroma, or intermetatarsal neuroma is a benign (non-cancerous) growth of nerve tissue (neuroma) that develops in the foot, usually between the third and fourth toes (an intermetatarsal plantar nerve, most commonly of the third and fourth intermetatarsal spaces). It is a common, painful condition.
Causes
Morton's Neuroma is a caused by pressure, abnormal function/motion or an imbalance in the structure of the foot such as flat feet, that causes an abnormal pressure on the structures and the nerves in the ball of the foot. It most commonly affects the nerve that goes to the 2nd 3rd or 4th toes. The squeezing of the nerve from abnormal motion leads to a protective thickening of the sheath that protects the nerve. Symptoms of Morton's Neuroma often occur during or after activities that cause a sidewards squeezing of the ball of the foot or from pressure such as walking, standing, or playing sport. Since squeezing is a common cause of the condition, shoes such as pointed toes or high heels can often lead to a neuroma. Shoes that are constricting, even tight sneakers, can pinch the nerve between the toes, causing inflammation and pain.
Symptoms
Typically, there's no outward sign of this condition, such as a lump. Instead, you may experience the following symptoms. A feeling as if you're standing on a pebble in your shoe. A burning pain in the ball of your foot that may radiate into your toes. Tingling or numbness in your toes. It's best not to ignore any foot pain that lasts longer than a few days. See your doctor if you experience a burning pain in the ball of your foot that's not improving, despite changing your footwear and modifying activities that may cause stress to your foot.
Diagnosis
A doctor can usually identify Morton's neuroma during a physical exam. He or she will squeeze or press on the bottom of your foot or squeeze your toes together to see if it hurts. Your doctor may also order an X-ray of your foot to make sure nothing else is causing the pain.
Non Surgical Treatment
Nonsurgical treatment is tried first. Your doctor may recommend any of the following. Padding and taping the toe area, shoe inserts, changes to footwear, for example wearing shoes with wider toe boxes or flat heels, Anti-inflammatory medicines taken by mouth or injected into the toe area, nerve blocking medicines injected into the toe area, other painkillers, physical therapy. Anti-inflammatories and painkillers are not recommended for long-term treatment. In some cases, surgery is needed to remove the thickened tissue and inflammed nerve. This helps relieve pain and improve foot function. Numbness after surgery is permanent.
Surgical Treatment
If these non-surgical measures do not work, surgery is sometimes needed. Surgery normally involves a small incision (cut) being made on either the top, or the sole, of the foot between the affected toes. Usually, the surgeon will then either create more space around the affected nerve (known as nerve decompression) or will cut out (resect) the affected nerve. If the nerve is resected, there will be some permanent numbness of the skin between the affected toes. This does not usually cause any problems. You will usually have to wear a special shoe for a short time after surgery until the wound has healed and normal footwear can be used again. Surgery is usually successful. However, as with any surgical operation, there is a risk of complications. For example, after this operation a small number of people can develop a wound infection. Another complication may be long-term thickening of the skin (callus formation) on the sole of the foot (known as plantar keratosis). This may require treatment by a specialist in care of the feet (chiropody).
Morton's neuroma, also called Morton's metatarsalgia, Morton's disease, Morton's neuralgia, Morton metatarsalgia, Morton nerve entrapment, plantar neuroma, or intermetatarsal neuroma is a benign (non-cancerous) growth of nerve tissue (neuroma) that develops in the foot, usually between the third and fourth toes (an intermetatarsal plantar nerve, most commonly of the third and fourth intermetatarsal spaces). It is a common, painful condition.Causes
Morton's Neuroma is a caused by pressure, abnormal function/motion or an imbalance in the structure of the foot such as flat feet, that causes an abnormal pressure on the structures and the nerves in the ball of the foot. It most commonly affects the nerve that goes to the 2nd 3rd or 4th toes. The squeezing of the nerve from abnormal motion leads to a protective thickening of the sheath that protects the nerve. Symptoms of Morton's Neuroma often occur during or after activities that cause a sidewards squeezing of the ball of the foot or from pressure such as walking, standing, or playing sport. Since squeezing is a common cause of the condition, shoes such as pointed toes or high heels can often lead to a neuroma. Shoes that are constricting, even tight sneakers, can pinch the nerve between the toes, causing inflammation and pain.
Symptoms
Typically, there's no outward sign of this condition, such as a lump. Instead, you may experience the following symptoms. A feeling as if you're standing on a pebble in your shoe. A burning pain in the ball of your foot that may radiate into your toes. Tingling or numbness in your toes. It's best not to ignore any foot pain that lasts longer than a few days. See your doctor if you experience a burning pain in the ball of your foot that's not improving, despite changing your footwear and modifying activities that may cause stress to your foot.
Diagnosis
A doctor can usually identify Morton's neuroma during a physical exam. He or she will squeeze or press on the bottom of your foot or squeeze your toes together to see if it hurts. Your doctor may also order an X-ray of your foot to make sure nothing else is causing the pain.
Non Surgical Treatment
Nonsurgical treatment is tried first. Your doctor may recommend any of the following. Padding and taping the toe area, shoe inserts, changes to footwear, for example wearing shoes with wider toe boxes or flat heels, Anti-inflammatory medicines taken by mouth or injected into the toe area, nerve blocking medicines injected into the toe area, other painkillers, physical therapy. Anti-inflammatories and painkillers are not recommended for long-term treatment. In some cases, surgery is needed to remove the thickened tissue and inflammed nerve. This helps relieve pain and improve foot function. Numbness after surgery is permanent.
Surgical Treatment
If these non-surgical measures do not work, surgery is sometimes needed. Surgery normally involves a small incision (cut) being made on either the top, or the sole, of the foot between the affected toes. Usually, the surgeon will then either create more space around the affected nerve (known as nerve decompression) or will cut out (resect) the affected nerve. If the nerve is resected, there will be some permanent numbness of the skin between the affected toes. This does not usually cause any problems. You will usually have to wear a special shoe for a short time after surgery until the wound has healed and normal footwear can be used again. Surgery is usually successful. However, as with any surgical operation, there is a risk of complications. For example, after this operation a small number of people can develop a wound infection. Another complication may be long-term thickening of the skin (callus formation) on the sole of the foot (known as plantar keratosis). This may require treatment by a specialist in care of the feet (chiropody).
Shoe Lifts The Chiropodists Treatment For Leg Length Discrepancy
There are two unique variations of leg length discrepancies, congenital and acquired. Congenital implies you are born with it. One leg is structurally shorter in comparison to the other. Through developmental periods of aging, the brain senses the step pattern and recognizes some variation. The body typically adapts by tilting one shoulder to the "short" side. A difference of under a quarter inch isn't really uncommon, require Shoe Lifts to compensate and typically doesn't have a profound effect over a lifetime.

Leg length inequality goes largely undiagnosed on a daily basis, however this issue is easily fixed, and can eliminate a number of instances of back problems.
Treatment for leg length inequality usually consists of Shoe Lifts. Most are affordable, in most cases being below twenty dollars, in comparison to a custom orthotic of $200 or more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Lower back pain is the most widespread condition afflicting men and women today. Around 80 million men and women experience back pain at some stage in their life. It is a problem which costs companies huge amounts of money yearly due to time lost and production. Fresh and superior treatment solutions are continually sought after in the hope of decreasing the economical impact this issue causes.

Men and women from all corners of the world experience foot ache as a result of leg length discrepancy. In a lot of these situations Shoe Lifts might be of very useful. The lifts are capable of decreasing any pain in the feet. Shoe Lifts are recommended by many qualified orthopaedic physicians.
To be able to support the body in a well-balanced manner, the feet have got a significant part to play. Irrespective of that, it can be the most neglected zone in the human body. Many people have flat-feet meaning there may be unequal force exerted on the feet. This causes other parts of the body including knees, ankles and backs to be affected too. Shoe Lifts make sure that suitable posture and balance are restored.
Leg length inequality goes largely undiagnosed on a daily basis, however this issue is easily fixed, and can eliminate a number of instances of back problems.
Treatment for leg length inequality usually consists of Shoe Lifts. Most are affordable, in most cases being below twenty dollars, in comparison to a custom orthotic of $200 or more. Differences over a quarter inch can take their toll on the spine and should probably be compensated for with a heel lift. In some cases, the shortage can be so extreme that it requires a full lift to both the heel and sole of the shoe.
Lower back pain is the most widespread condition afflicting men and women today. Around 80 million men and women experience back pain at some stage in their life. It is a problem which costs companies huge amounts of money yearly due to time lost and production. Fresh and superior treatment solutions are continually sought after in the hope of decreasing the economical impact this issue causes.
Men and women from all corners of the world experience foot ache as a result of leg length discrepancy. In a lot of these situations Shoe Lifts might be of very useful. The lifts are capable of decreasing any pain in the feet. Shoe Lifts are recommended by many qualified orthopaedic physicians.
To be able to support the body in a well-balanced manner, the feet have got a significant part to play. Irrespective of that, it can be the most neglected zone in the human body. Many people have flat-feet meaning there may be unequal force exerted on the feet. This causes other parts of the body including knees, ankles and backs to be affected too. Shoe Lifts make sure that suitable posture and balance are restored.
What Are The Primary Causes Of Heel Spur

Overview
Heel spurs are a relatively common cause of heel pain. A heel spur is a pointed bone fragment that extends forward from the bottom of the heel from the heel bone, also referred to as a calcaneous. Serious pain and discomfort often develops with this condition. In many cases, a heel spur develops along with plantar fasciitis which occurs when the plantar fascia ligament becomes inflamed.
Causes
Bone spurs form in the feet in response to tight ligaments, to activities such as dancing and running that put stress on the feet, and to pressure from being overweight or from poorly fitting shoes. For example, the long ligament on the bottom of the foot (plantar fascia) can become stressed or tight and pull on the heel, causing the ligament to become inflamed (plantar fasciitis). As the bone tries to mend itself, a bone spur can form on the bottom of the heel (known as a ?heel spur?). Pressure at the back of the heel from frequently wearing shoes that are too tight can cause a bone spur on the back of the heel. This is sometimes called a ?pump bump,? because it is often seen in women who wear high heels.

Symptoms
Heel spurs result in a jabbing or aching sensation on or under the heel bone. The pain is often worst when you first arise in the morning and get to your feet. You may also experience pain when standing up after prolonged periods of sitting, such as work sessions at a desk or car rides. The discomfort may lessen after you spend several minutes walking, only to return later. Heel spurs can cause intermittent or chronic pain.
Diagnosis
The diagnosis of heel pain and heel spurs is made by a through history of the course of the condition and by physical exam. Weight bearing x-rays are useful in determining if a heel spur is present and to rule out rare causes of heel pain such as a stress fracture of the heel bone, the presence of bone tumors or evidence of soft tissue damage caused by certain connective tissue disorders.
Non Surgical Treatment
A conventional treatment for a heel spur is a steroid injection. This treatment, however, isn?t always effective because of the many structures in the heel, making it a difficult place for an injection. If this treatment goes wrong, it can make the original symptoms even worse. Another interesting means of treatment is Cryoultrasound, an innovative electromedical device that utilizes the combination of two therapeutic techniques: cryotherapy and ultrasound therapy. Treatments with Cryoultrasound accelerate the healing process by interrupting the cycle and pain and spasms. This form of therapy increases blood circulation and cell metabolism; it stimulates toxin elimination and is supposed to speed up recovery.
Surgical Treatment
Surgery, which is a more radical treatment, can be a permanent correction to remove the spur itself. If your doctor believes that surgery is indicated, he will recommend an operation - but only after establishing that less drastic methods of treatment are not successful.
Prevention
Heel Spur symptoms can be prevented from returning by wearing proper shoes and using customized orthotics and insoles to relieve pressure. It is important to perform your exercises to help keep your foot stretched and relaxed.
What Can Induce Heel Spur

Overview
While the term heel spur may create the impression of a sharp bony projection on the bottom of the heel that pokes the bottom of our foot causing our pain. Painful heel spurs are actually a result of damage to the soft tissue at the bottom of the foot. While this may be confusing, we'll try to explain. Heel spurs is the more common name for a condition that is medically referred to as plantar fascitiis or heel spur syndrome. Plantar fasciitis is a location oriented term that refers to the bottom of the foot(i.e. plantar warts). Fascia is a tough, inelastic band. 'itis'is a term used to describe something that is inflamed (i.e. tendonitis, bursitis).
Causes
This condition is a constellation of many causes; overweight, ill fitting shoes, bio-mechanical problems (mal-alignment of the heel), gout, pronation (a complex motion including outward rotation of the heel and inward rotation of the ankle) and rheumatoid arthritis are some of the causes of heel pain.

Symptoms
Most of the time heel spurs present as pain in the region surrounding the spur, which typically increases in intensity after prolonged periods of rest. Patients may not be able to bear weight on the afflicted heel comfortably. Running, walking, or lifting heavy weight may exacerbate the issue.
Diagnosis
A thorough history and physical exam is always necessary for the proper diagnosis of heel spurs and other foot conditions. X rays of the heel area are helpful, as excess bone production will be visible.
Non Surgical Treatment
Perform some exercises. Exercises that strengthen and lengthen your plantar fascia can also be very helpful for heel spurs. Try some of the following activities. Calf stretch. Place your hands on a wall. Extend 1 foot (0.3 m) behind you with your knee straight and place the other foot in front of you with the knee bent. Push your hips toward the wall and hold the stretch for 10 seconds. You should feel a pull in your calf muscles. Repeat the stretch 20 times for each foot. Plantar fascia stretch, Perform this exercise in the morning before you've done any standing or walking. Cross your injured foot over the knee of your other leg. Grasp your toes and gently pull them toward you. If you can't reach your toes, then wrap a towel around them and pull on the towel. Hold the stretch for 10 seconds and repeat 20 times for each foot.
Surgical Treatment
More than 90 percent of people get better with nonsurgical treatments. If conservative treatment fails to treat symptoms of heel spurs after a period of 9 to 12 months, surgery may be necessary to relieve pain and restore mobility. Surgical techniques include release of the plantar fascia, removal of a spur. Pre-surgical tests or exams are required to identify optimal candidates, and it's important to observe post-surgical recommendations concerning rest, ice, compression, elevation of the foot, and when to place weight on the operated foot. In some cases, it may be necessary for patients to use bandages, splints, casts, surgical shoes, crutches, or canes after surgery. Possible complications of heel surgery include nerve pain, recurrent heel pain, permanent numbness of the area, infection, and scarring. In addition, with plantar fascia release, there is risk of instability, foot cramps, stress fracture, and tendinitis.